CLEVER: A Framework for Connecting Lived Experiences with Visualisation of Electronic Records
Mai Elshehaly, Lucy H Eddy, Mark Mon-Williams
Room: 104
2023-10-25T05:30:00ZGMT-0600Change your timezone on the schedule page
2023-10-25T05:30:00Z
Fast forward
Full Video
Keywords
Human-centered computing—Visualization—Visualization design and evaluation methods
Abstract
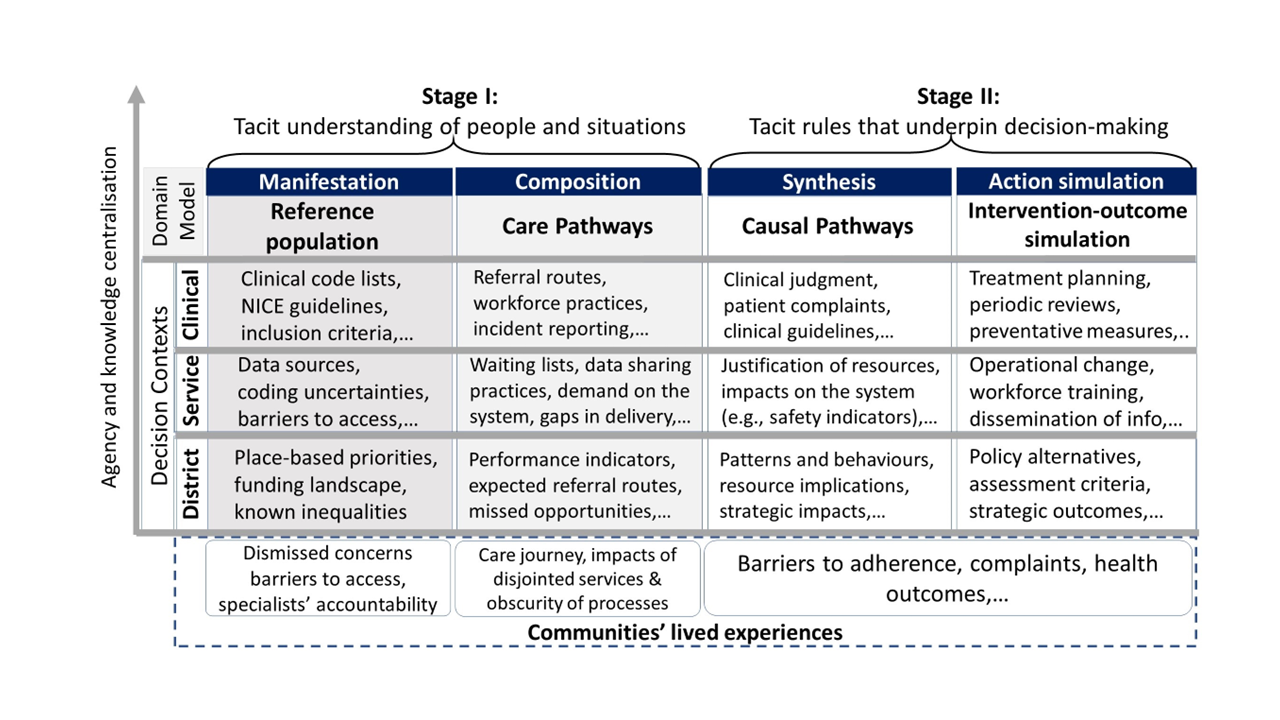
The disconnect between insights generated from data and real-life practices of decision makers presents a number of open questions for visual analytics (VA). In public service planning, routine data are often perceived as unavailable, biased, incomplete and inconsistent across services. Decision makers often rely on qualitative data - sometimes collected through co-production - to understand the lived experience of communities before formulating a decision. We followed a subjectivist case study approach and immersed ourselves in ongoing co-production activities over the course of one year, to capture how VA can support the dialogue between population health decision-makers and the communities they serve. We present a framework for Connecting Lived Experiences with Visualisation of Electronic Records (CLEVER). The framework regards visualisation as a central component in a complex adaptive decision-making ecosystem and highlights the need to structure domain knowledge across decision contexts in Population Health Management (PHM) at clinical-, service- and district-levels. Our process for developing an initial framework comprised three steps: (i) we elicited decision-making tasks through a series of qualitative data collection activities; (ii) we developed a preliminary domain model to capture data views and a subjective view of the world through human stories; and (iii) we developed a series of visualisation prototypes to instantiate the framework and demonstrated them regularly to stakeholders. In future work, we will conduct ‘deep dives’ to systematically study the role of VA in individual stages of the framework.